Hanaa A. Fatoum, MBBS1, Kat Kuzmeskas, MPH2, John D. Halamka, MD, MS3, Shahrukh K. Hashmi, MD, MPH4,5
Affiliations: 1College of Medicine, Alfaisal University, Riyadh, Saudi Arabia; 2Tamarin Health, Brighton, MA, USA; 3Mayo Clinic Platform, Mayo Clinic, Rochester, MN, USA; 4Department of Medicine, Mayo Clinic, Rochester, MN, USA; 5Sheikh Shakhbout Medical City, Mayo Clinic, Abu Dhabi, UAE
Corresponding Author: Shahrukh K. Hashmi, MD, MPH; Email: hashmi.shahrukh@mayo.edu
Keywords: Blockchain, COVID-19, Machine-Learning, Pandemic, Point-of-Care Testing, Serology-Based Test, Test
Section: Discussion
The last catastrophic pandemic the world has seen was the 1918 H1N1 influenza pandemic, considering that it happened 102 years ago, one can perhaps leverage the technologic advancements over the past century to combat the current pandemic of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (COVID-19), which has already infected more than 16 million people globally and shut down the majority of the daily activities of life. The danger and challenge of infectious diseases such as COVID-19 lies in their highly contagious nature, spreading like wildfire with the potential to infect the majority of the world’s population unless drastic measures are undertaken. In some countries, the social distancing and quarantine measures are either insufficient or ineffective as the number of cases is still on the rise. A major issue causing this rise is that most COVID-19 carriers appear asymptomatic. Identifying infected individuals as well as healthy/immune ones is the most crucial step in halting the disease spread. This is where the role of mass screening comes in.
There are currently two main methods for COVID-19 testing: molecular (detection of the viral ribonucleic acid through polymerase chain reaction [PCR]) and serology- (immunoglobulin G [IgG] and immunoglobulin M [IgM] antibodies) based. The PCR has a slow turnaround, is labor-intensive, and requires sophisticated laboratory machines, making it more suitable for high risk and severely symptomatic patients, whereas the serologic-based testing is relatively inexpensive, fast, convenient, and ideal for point-of-care testing (POCT) and mass screening for COVID-19, including asymptomatics. While many companies are trying to produce new, high-quality, rapid testing kits such as lateral flow immunoassays, the United States Food and Drug Administration only recently approved the first rapid serology-based test. While antibodies testing is pivotal in the response to the pandemic, one crucial part of the buzzle puzzle remains unclear. That is, which is whether immunity occurs postinfection and if so, for how long. The detection and interpretation of the presence and levels of various serum antibodies is a key for easing the lockdown measures, reopening borders, and restoring daily activities.
For mass screening, POCT can allow vast diagnostic testing at or near patients’ sites and may include emergency departments, primary care settings, outreach clinics, and mobile settings. Efficient utilization of mass screening was exhibited by authorities in Vó (a small town in Italy). Researchers implemented the mass-testing strategy with the majority of Vó’s 3,000 inhabitants after the lockdown. This allowed researchers to identify and isolate those who tested positive, including many asymptomatic carriers, eventually halting the spread of COVID-19. Another technologic advancement that can be harnessed at mass scale in pandemics due to contagions is wearable devices or the Internet of Things, which may include body-temperature sensors. For SARS-CoV-2, such sensors are particularly useful since high-grade fever is a hallmark of the COVID-19 disease.
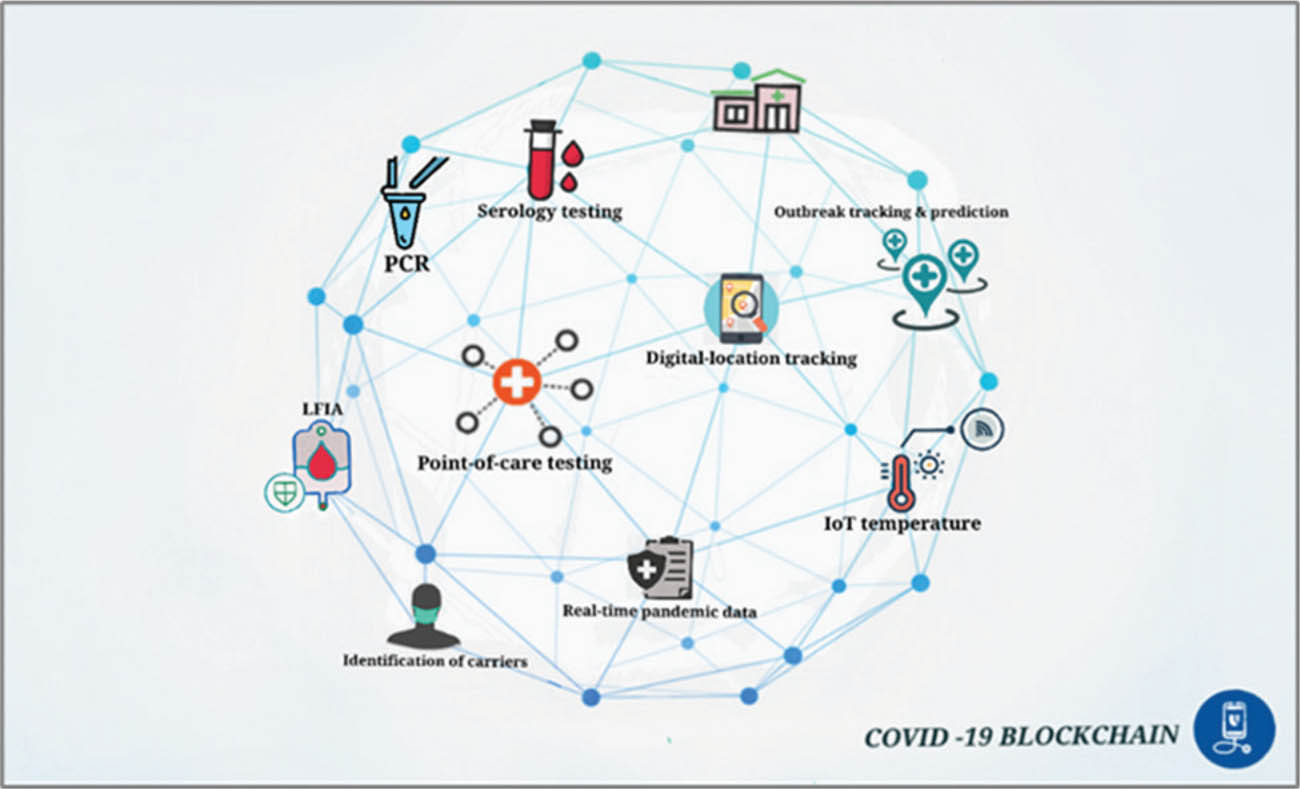
Regardless of the screening methodology used, the obvious question is how to operationalize current technological advancements to control the pandemic on a global scale. Managing data from testing and sensors, while maintaining coordination between authorities, hospitals, governments, and various POCT facilities—at mass scale—without compromising privacy and security is challenging. This is where blockchain technology can be of great value. Blockchain is a distributed ledger technology, where there is no central authority over the data. It enables secure, trustless, and reliable real-time storage and sharing of unalterable data, which could serve as the backbone for a health passport. Using a blockchain to create a health passport that stores COVID-19 test results and is available readily for information at institutions and governmental agencies is a viable avenue to curbing the spread of COVID-19 on a mass scale. The contents of the passport are backed by a blockchain, so there is verifiable proof that the results were not tampered with by any party. Similarly, for the frontline healthcare staff, knowing who is COVID-19 immune via the health passport can be a game-changer in combatting the disease and treating the affected patients while protecting healthcare workers. The blockchain-based passport can be taken a step further by using the test results in conjugation with digital mobile location tracking services, powered by machine learning (ML) models, to identify the disease hotspots, patterns of spread, and alert individuals who have been in contact/proximity from those who have tested positive for the disease as soon as their test results go on the blockchain (Figure 1).
Figure 1—The blockchain-based passport.
Some governments and organizations are already planning to employ blockchains and ML algorithms for combatting this outbreak. Specifically, the World Health Organization has recently launched its blockchain-based COVID-19 platform called MiPasa. “It is a global-scale control and communication system that enables a swift and more precise early detection of COVID-19 carriers and infection hotspots through seamless and fully private information sharing between individuals, state authorities and health institutions such as hospitals and HMOs (health maintenance organizations), utilizing advanced technological tools and a dedicated user app, outsmarting COVID-19 using Crowd Data (the Intelligence of the Crowd), and can also help monitor and foresee local and global epidemiological trends and detect likely asymptomatic carriers by feeding big data on infection routes and occurrences to powerful artificial intelligence-based processors globally.”4 Another blockchain implementation that can be useful without the need for contact tracing, location data tracking, or storing sensitive data on-chain, which all carry significant privacy and policy implications, would be a blockchain-backed Unique Testing ID. There lacks a unified national and international response to the pandemic. Each state and nation implemented their own pandemic response. In addition, there is no unifying identity to leverage across borders that shares COVID-19 infection or immunity status. A testing passport that has a Unique Testing ID for the individual can provide the necessary data without compromising unnecessary protected information.
A blockchain architecture that uses on-chain smart contracts to interact with data off-chain is one the most effective methods for protecting privacy, as well as reducing data traffic, and could form the architecture of the Unique Testing ID. A framework proposed by MIT Media Lab researchers called MedRec5 defines this infrastructure. The researchers used different layers of blockchains (a public-permissioned blockchain) and their respective smart contracts in order to securely govern access to data. Implementing this technology for a COVID-19 Unique Testing ID would involve a smart contract-based key pair system or an ID contract (IDC) that links an existing form of ID, such as a passport number or a social security number, to their respective Unique Testing ID. Then, a permissioned testing contract (TC) would function as a trustless, uniform, and private data storage ledger for all testing data from various facilities. These two would communicate via a mediation contract, which retrieves testing information, acting as a mediator between the IDC and TC blockchain without compromising neither the patient privacy nor the trustlessness (integrity) of the data.
Finally, it is of utmost importance to protect the privacy of patients and their data when applying digital solutions as well as maintain the integrity of the data, which is another advantage of blockchain; yet, certain limitations of blockchains should be addressed. The blocks are not 100% immune to privacy breaches, and the scalability issues matter when dealing with massive amounts of global megadata on a public blockchain. However, disease outbreak such as COVID-19 is a good example to test the power of blockchains, especially public-permissioned and a key pair system, which can be global, rapid, and potentially harness real-time data to merge efforts, improve coordination, and combat any pandemic at both governmental and nongovernmental levels.
We hope that the focus on technological advancements will serve as a call for the implementation of a blockchain-based mass testing strategy to eradicate COVID-19.
None of the authors declare any relevant conflicts of interest.
SKH has received funding from Mallinckrodt, Pfizer, Novartis, and Janssen. SKH has received travel grants from MSD (Merck Sharp & Dohme), Takeda, Gilead, and BMS (Bristol Myers Squibb).
All authors approved the final version of the draft. HF created the figure.
| 1. | 1918 Pandemic (H1N1 virus) | Pandemic influenza (flu) | CDC. Cdc.gov.; 2020 [cited 2020 Apr 03]. Available from: https://www.cdc.gov/flu/pandemic-resources/1918-pandemic-h1n1.html |
| 2. | Emergency Use Authorizations. U.S. Food and Drug Administration. 2020 [cited 2020 Apr 05]. Available from: https://www.fda.gov/medical-devices/emergency-situations-medical-devices/emergency-use-authorizations |
| 3. | Tondo L. Scientists say mass tests in Italian town have halted Covid-19 there. The Guardian. 2020 [cited 2020 Apr 05]. Available from: https://www.theguardian.com/world/2020/mar/18/scientists-say-mass-tests-in-italian-town-have-halted-covid-19 |
| 4. | What is MiPasa—MiPasa. MiPasa. 2020 [cited 2020 Apr 05]. Available from https://mipasa.org/about/ |
| 5. | Azaria A, Ekblaw A, Vieira T, Lippman A. MedRec: Using blockchain for medical data access and permission management, 2016. 2nd International Conference on Open and Big Data (OBD). Vienna, 2016; p. 25–30 [cited 2020 Oct 31]. Available at https://ieeexplore.ieee.org/document/7573685/citations?tabFilter=papers#citations |
Copyright Ownership: This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.