Will Abramson,1 Dr Nicole E. van Deursen,2 William J Buchanan1
Affiliations: 1Blockpass ID Lab, School of Computing, Edinburgh Napier University, Edinburgh, UK; 2National Cyber Security Centre, The Hague, The Netherlands, Edinburgh Napier University, Edinburgh, UK
Corresponding author: William J Buchanan, Blockpass ID Lab, School of Computing, Edinburgh Napier University, Edinburgh. w.buchanan@napier.ac.uk
Keywords: Digital Credentials, Trust, Healthcare, Passporting, SSI, Design
Section: Original Clinical Research
A substantial administrative burden is placed on healthcare professionals as they manage and progress through their careers. Identity verification, pre-employment screening, and appraisals: the bureaucracy associated with each of these processes takes precious time out of a healthcare professional’s day. Time that could have been spent focused on patient care. In the midst of the COVID-19 crisis, it is more important than ever to optimize these professionals’ time. This article presents the synthesis of a design workshop held at the Royal College of Physicians of Edinburgh (RCPE) and subsequent interviews with healthcare professionals. The main research question posed is whether these processes can be re-imagined using digital technologies, specifically self-sovereign identity? A key contribution in the article is the development of a set of user-led requirements and design principles for identity systems used within healthcare. These are then contrasted with design principles found in the literature. The results of this study confirm the need and potential of professionalizing identity and credential management throughout a healthcare professional’s career.
While the COVID-19 crisis has brought the challenges of staff mobility into the spotlight, the administrativ e burden placed on a healthcare professional throughout their career has always been present. Over the years, healthcare service providers have increased the minimum standard for identity verification and pre-employment checks in line with new regulations.1,2 As a result, the time spent on these processes has increased. A House of Lord’s report, for example, estimated that 25,000 junior doctor days a year were currently being spent on these administrative tasks.3 In addition to this, digitization of healthcare services has further increased the time and complexity associated with managing one’s career. In a 2011 US survey, 87% of physicians stated that the leading cause of stress was down to administration,4 and a study of Finnish physicians found that poorly functioning IT systems continue to be a major cause of stress, particularly for those in highly time pressured roles.5
In a crisis like the COVID-19 outbreak, the need for a healthcare service to react to rapidly evolving, location-specific stresses at a trust or hospital level cannot be clearer. Different locations may hit their peak at different times, while some areas may only be minimally affected.6 However, consultation with a Royal College of Physicians of Edinburgh (RCPE) trainee suggests that on-boarding into a new trust or hospital can take up to 2 days. This is 2 days of precious time that could potentially have been spent saving lives. Technological solutions have regularly been heralded for their ability to reduce inefficiencies and streamline patient care. Blockchain technology is just one of the more recent innovations predicted to have a disruptive impact.7
Often though, the reality in the hospitals is different to the design assumptions made by technologists, and the productivity benefits are not always obvious.8
This article thus presents an initial set of design principles for any technical solution attempting to reduce the administrative burdens currently placed on healthcare professionals. An analysis of discourse about digital identities, verifiable claims, and trust has led to a theoretical set of trust and design principles. These principles were validated in a workshop with healthcare organizations held at the RCPE. This research takes an initial step towards understanding the problem space from the perspective of those currently experiencing it and lays the foundation for future quantitative studies in this area.
This article evaluates a use case in which a person can digitally obtain, manage, and present his/her professional credentials and personally identifiable data within an healthcare system. We limited the scope of the work to healthcare professionals, as these are identified as being burdened with administrative tasks associated with identity verification and pre-employment checks, as well as recording and managing their credentials as they progress through their career, a burden which is generally expected to take place in people’s personal lives. The following research questions were identified:
Berwick, Nolan, and Whittington define the Triple Aim focusing on improving the care, health, and cost when accessing healthcare performance in the United States.9 They point out that these goals are interdependent so must be considered together when planning and evaluating healthcare changes. It has been suggested that this framework should be extended to consider a fourth aim, care for the provider,10 due to reports that staff burnout and dissatisfaction are widespread. As care providers are on the frontline when it comes to achieving the triple aim for healthcare services, including their well-being into this assessment makes sense.
Healthcare providers have a requirement to maintain strong identity verification checks to ensure that their employees are who they claim to be and that they have the required skills and training for the job.2,11,12 Unfortunately, there have been examples throughout the world of doctors practicing without licenses. This puts patients’ lives at risk and reduces the trust in the profession as a whole. Examples include the UK General Medical Council recently having to recheck credentials of 3,000 doctors after a fraudulent psychiatrist was found to have practiced for 23 years without proper credentials,13 the case of a social worker in Canada involved in more than 100 child protection cases,14 and the notorious US case of Christopher Duntsch a.k.a Dr Death.15
As a consequence, credentialing healthcare professionals is a crucial process in healthcare systems throughout the world. However, the current practices of many systems add huge overheads to both the administrators and the healthcare professionals. In a report on healthcare and digital credentials, the US Federation of State Medical Boards (FSMB)11 analyze the use of digital credentials in healthcare, looking at the potential for both current technology and future technology to streamline the process and enhance trust in the system. The implementation of the Federation Credentials Verification Service (FCVS) in 1996,16 an NCQA-certified platform providing a centralized service for obtaining primary source, verified education information for medical practitioners applying for licensing in the United States. As the report11 outlines, the FCVS reduced the time to obtain a license from 60 days to 25 days, a significant reduction. However, efforts to improve the FCVS highlighted the underutilization of technology in the process. Furthermore, 66% of this time is driven by parties outside of the control of the FCVS.11 These credential verification organizations are often redundant and increase the cost of the whole process. The report highlights the movement to disintermediate the creation and management of credentials, hinting at a movement toward individual ownership of credentials.
Along with this, there is an increasing need for clinical staff to provide digital evidence of their training, skills, and experience. Read et al.17 investigated the usage of a passporting system for surgery clerkship and found that those involved often found that it improved student’s reporting of their performance in basic clinical skills.
Digital identifiers—and the trust entities place in them—enable many modern societal interactions. They thus allow organizations to perform critical activities with increased levels of trust. Another way of looking at it is from a risk perspective and where digital identifiers and account information correlated with an identifier that helps organizations make risk-based decisions associated with a particular interaction and value exchange. Unfortunately, traditional identity management systems continue to have security risks,18 such as:
credential theft or loss, biometric impersonation, document forgery, and identity theft.
SSI uses a new type of identifier currently going through standardization at the W3C, a decentralized identifier (DID).19 A DID is an identifier under the sole domain of an entity, typically the entity that created it. It is cryptographically verifiable and independent of any central authority. Rather than being assigned an identifier on account creation, DIDs let individuals provide their own identifiers for their digital relationships.
Systems built following an SSI architecture could offer the opportunity to rethink the entire credential process for physicians. Before the electronic transmission of credentials can be put forward as a viable option for healthcare professionals, it must be considered if such a process would break any of the rules and regulations currently governing this area. The key things identity verification and authentication process must satisfy for most healthcare services are2,11:
These points can, in fact, all be satisfied digitally through the use of digital signatures.
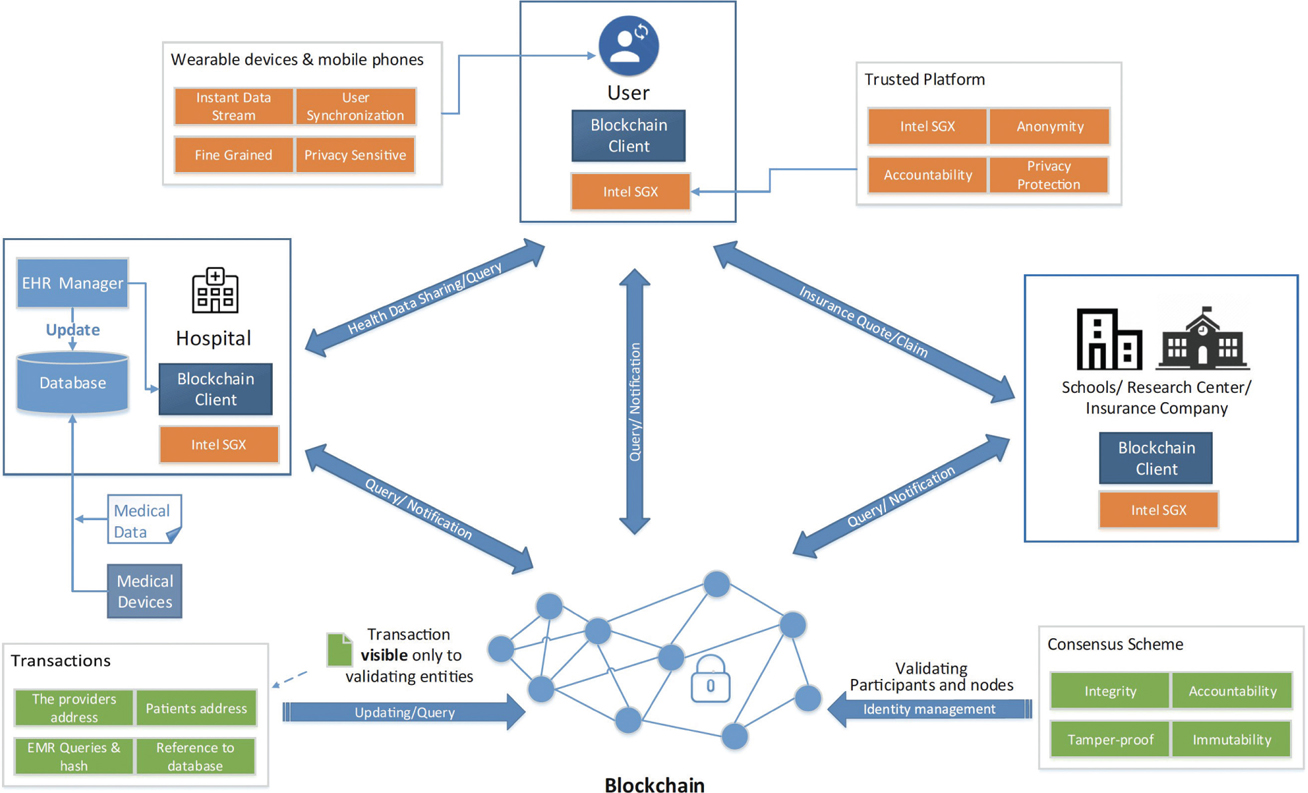
The problem of scaling digital identities into healthcare systems has led many people to explore alternative methods to identify and authenticate people and things in the digital sphere. One of the proposed architectures is commonly referred to as self-sovereign identity (SSI). Connor-Green identifies that SSIs could be one of the core use cases of blockchain in health.20 Liang et al. outline a blockchain approach within a healthcare management system, where the distributed nature of SSIs supports a scalable infrastructure that moves away from the centralized control of identity within many existing healthcare infrastructures (Figure 1).21,22
Figure 1—Patient-centric personal health data management system.21
The goal of the workshop was to gather a set of values and principles that can be used to evaluate emerging technology for identity systems within healthcare. Terminology and definitions are often much contested in different contexts. We used definitions provided in the selected papers as much as possible, but some definitions were adapted to better fit our goal to measure the value or principle.
The next step in our research was a workshop organized at RCPE. It involved 14 participants with a wide ranging experience of different aspects of the healthcare system. The participants for the workshop were selected through consultation with the RCPE, and who were able to use their contacts to invite a diverse range of attendees. This included clinicians, RCPE trainees, and RCPE staff involved in data management, digital transformation, and education, as well as a representative from the General Medical Council (GMC). While no personal data was captured during the workshop and all attendees remain anonymous, explicit consent was obtained and the research aims were explained at the beginning of the workshop.
During the workshop, the participants evaluated the fit of SSI within the healthcare domain. First, a process mapping exercise was used to develop an understanding of the current system, looking at the identity data exchanges and key entities that verify or attest to identity attributes of healthcare professionals throughout their career.
Then, these identity moments were re-imagined within an SSI-enabled ecosystem, and this story was told in an interactive manner using physical props and audience participation in order to convey the capabilities that SSI systems could provide for healthcare professionals, without going into unnecessary technical detail. Finally, the workshop participants were asked to evaluate the positive and negative aspects of the identity management system. The participants expressed their requirements, values, and expectations. The list that was distilled from these workshop discussions was compared against the list of design principles from the desk research.
The success of any SSI system depends not only on the technical feasibility but also on the user acceptance and trust in the system. With users we mean all stakeholders (entities) within a specific context that will use that system together. Trust is harder to define, as there exist more than 70 definitions in academic literature.23 Trust is seen as a human strategy
to cope with uncertainty, such as those we face in relations, actions, and innovation.24 In a digital context, trust is often transferred to cybersecurity measures such as technological controls, certificates, and organizational compliance frameworks. In SSI systems, at least some aspects of this trust shifts from trust between people toward confidence that is placed in cryptographic systems. As Smolenski25 frames it: trust is being depersonalized. Designing new digital identity systems means mimicking real-life situations in a digital way. Human values, such as ethics and trust, need a digital equivalent that users need to accept and understand. How do we design trust from the start? Which design principles are most valued by users and most likely to establish trust in these systems?
There are many papers that refer to the Laws of Identity (coined by Cameron in 2005)26 as the foundation for design principles. These laws explain the dynamics causing digital identity systems to succeed or fail in various contexts. Although written before the era of SSI, Cameron himself finds the laws still relevant, also for identity systems on the blockchain and decentralized identity.27 He points out, for instance, that the first four of the laws are also requirements within the GDPR.
In 2016, Christopher Allen28 wrote 10 principles inspired by (among others) the work of Cameron. His aim was to ensure that user control is at the heart of SSI. Allen pointed out that identity can be a double-edged sword: it can be used for both beneficial and maleficent purposes. Therefore, he states: an identity system must balance transparency, fairness, and support of the commons with protection for the individual. The Sovrin Foundation29 adopted Allen’s principles and arranged them in three sections, but this causes some confusion as they used one principle twice and made another principle a section above other principles. Other researchers and developers have used Cameron’s or Allen’s principles for inspiration and adapted them to their own lists of features. However, testing of SSI systems against these features and design principles is still rare.
Dunphy and Petitcolas30 evaluated three identity management solutions (uPort, Sovrin, and ShoCard) against Cameron’s laws of identity. Their overview shows that none of the solutions meets all seven laws, and none of them meets the law of human integration: usability, user understanding, and user experience. They state that none of the schemes they evaluated are accompanied by an evidence-based vision of user interaction. One of the limitations is usable end-user key management for nontechnical users that remains unaddressed. Furthermore, they express concern about tightening regulation, such as the GDPR, that sometimes contradicts the transparency of data storage in these solutions. Finally, most solutions provide only ad hoc trust, as trust relies on integration between participating entities, and methods to achieve trust in the context of identity attributes are still evolving.
Ferdous et al.31 elaborated on the principles of Allen and designed a taxonomy of essential properties for SSI. Then, they compared four blockchain-based SSI systems (uPort, Jolo, Sovrin, Blockcerts) against the properties, and through desk research, they found that most of the systems satisfy most of the properties. Similar work was done in a student project32 where students compared eight blockchain-based (IDchainz, Uport, EverID, Sovrin, LifeID, Selfkey, Shocard, Sora) and three non-blockchain-based SSI systems (PDS, IRMA, reclaimID) against each of Allen’s principles with one additional principle.33 They concluded that some of the blockchain-based solutions fulfill all properties, but that some of the non-blockchain-based implementations meet most of the criteria as well. Interestingly, their conclusions as to whether the properties are met do not always match the conclusions of Ferdous et al.31 for two systems (Uport and Sovrin) that both projects evaluated. Toth and Anderson-Priddy34 validated nine properties from earlier sources (e.g., Allen and Sovrin Foundation) and added new properties. They applied these properties to their architecture for digital identity and reasoned how these apply to their solution (NexGenID).
To the best of our knowledge, published evaluation of values and principles with users in a specific SSI context is very rare. One project that focused on citizens and digital identity systems in general (not SSI specific) was the Digital Identity lab in the Netherlands. In several interactive sessions with citizens, they found which values matter the most for digital identities.35 The research methods included interviews in the streets, meet-ups, expert sessions, and design sprints. The results include evaluation quadrants to plot digital identity providers and an overview of values that citizens find important and that can be used as input for ethical design and trust of digital identity systems. Another project focusing on user experience is the IRMA Made Easy project.36 IRMA (I Reveal My Attributes) is a self-sovereign identity solution with a digital wallet. The IRMA Made Easy Project works on the design of the app and website with a focus on accessibility. The developers of IRMA point out that user experience design affects how users handle the control over their information. From their experience, they share three lessons:
From the literature study, we learned that there is a gap in academic research that includes evaluation of proposed SSI solutions from a user perspective with domain knowledge of the ecosystem. Furthermore, to the best of our knowledge, the most commonly used design principles have not been validated by users for importance and priority. Projects that included consumers focus on identity management in general, and studies on SSI systems tend to focus on the evaluation by technical experts through desk research. Furthermore, when SSI design principles and features indeed are evaluated, the researchers re-use existing frameworks or lists of principles without user elicitation for principles that technology experts have not imagined yet. If we do not understand the requirements of end users, then we run the risk of creating digital tools that no one wants to use, or worse introducing unintended consequences through the deployment of these systems to domains with poorly understood requirements. There are countless examples of technology being introduced into healthcare only to make the jobs of those working alongside this technology worse, like the 15 logins needed to access different NHS systems.37
We compared the different lists of principles, features, and values that we found and created an overview of different and overlapping principles. The results are presented in Table 1. The overview of principles was input for the next stage in our research, where we invited future users to express their opinion on principles and values. In the next section, we describe the workshop that we held with representatives of different entities in an ecosystem, in order to contribute to the knowledge of end-user perception and trust of SSI systems.
Table 1. List of design principles.
| Cameron26 | Allen28 | Ferdous et al.31 | De Waag35 | Toth Anderson Priddy34 |
|---|---|---|---|---|
| Existence | Existence | |||
| User Control and Consent | Control and Consent | Consent | Control | Control and consent |
| Access | Access | Access | Access | |
| Transparency | Transparency | Transparency | ||
| Pluralism of operators and technologies | Portability | Portability | Portability | |
| Consistent experience across contexts | Interoperability | Interoperability | Interoperability | |
| Persistence | Persistence | Persistence | ||
| Minimal disclosure for a constrained use | Minimalization | Minimalization | Data-minimalization | |
| Protection | Protection | Security | Secure transactions and identity transfer | |
| Autonomy | Autonomy | |||
| Justifiable parties | Choosability | |||
| Human integration | Ease of use | Usability | ||
| Disclosure | ||||
| Ownership | ||||
| Directed identity | Single source | |||
| Standard | ||||
| Cost | ||||
| Availability | ||||
| Trust | ||||
| Privacy | ||||
| Integrity | ||||
| Decentralization | ||||
| Inclusivity | ||||
| Reliability | ||||
| Counterfeit prevention | ||||
| Identity verification | ||||
| Disclosure | ||||
| Identity assurance |
Table 2. The list of design principles was validated in a workshop.
| Design Principle | Definition |
|---|---|
| Existence | The identity of a person exists independent of identity administrators or providers. Control: The person is in control of their digital identity and is able to choose what personal data to share. |
| Autonomy | A user is independent on creating identities, as many as required, without relying on any party and be able to update/remove it. |
| Disclosure | A user must have the ability to selectively disclose particular attributes. |
| Ownership | The user is the ultimate owner of an identity, including the claims. |
| Consent | Data must be released only after the user has consented to do so. |
| Access | The person has full access to their own data. |
| Single source | A user is the single source of truth regarding the identity. |
| Transparency | Systems and algorithms are transparent and anyone should be able to examine how they work. |
| Standard | An identity must be based on open standards. |
| Cost | Costs must be kept to minimum. |
| Portability | Information and services about identity must be transportable to other services. |
| Interoperability | Digital identities are continually available and as widely usable as possible. |
| Persistence | An identity must be persistent as long as required by its owner. |
| Minimalization | When data is disclosed, that disclosure should involve the minimum amount of data necessary to accomplish the task at hand. For example, if only a minimum age is called for, then the exact age should not be disclosed, and if only an age is requested, then the more precise date of birth should not be disclosed. |
| Protection | The rights of users must be protected. When there is a conflict between the needs of the identity network and the rights of individual users, then the network should err on the side of preserving the freedoms and rights of the individuals over the needs of the network. |
| Availability | An identity must be available and accessible from different platforms when required by its owner. |
| Human welfare | The identity system must contribute to human well-being. |
| Non-maleficence | The system will not cause harm to others. |
| Justice | Systematic unfairness (false negatives/positives) is avoided. |
| Trustworthiness | Expectations to act with good will towards others. |
| Privacy | The user has the right to decide what data is shared and to set boundaries. |
| Dignity | Dignity is intertwined with emotional identity. Technological solutions have a responsibility to uphold human dignity. |
| Solidarity | Respectful cooperation between stakeholders. |
| Environmental welfare | The solution should cause no environmental harm. |
After a brief introduction, participants were asked to complete a warm up exercise where they recorded different identity interactions that occur throughout a typical day in their life. This included using a RFID card, logging into a digital system with a username and password, and authenticating to a mobile device, bank card payments, anything that involved some form of identification and authentication. Participants were also asked to record times when authentication failed, for example, through a rushed or forgotten password attempt.
The aim of the exercises was to get attendees thinking about how often they interact with digital systems, how many different username and passwords they currently manage, and the number of different authentication devices that they have to carry. The majority of participants recorded over 25 separate identity interactions, all in a single day.
The next stage of the workshop focused on eight core identity moments that captured at a high level the typical experiences of a doctor throughout their career. Participants were asked to create process maps identifying key organizations involved in each of these stages and the identity information that a doctor is required to present to them. Additionally, participants were asked to capture frustrations that a doctor might experience while navigating these identity moments. The general identity moments identified and validated prior to the workshop to provide some structure were as follows:
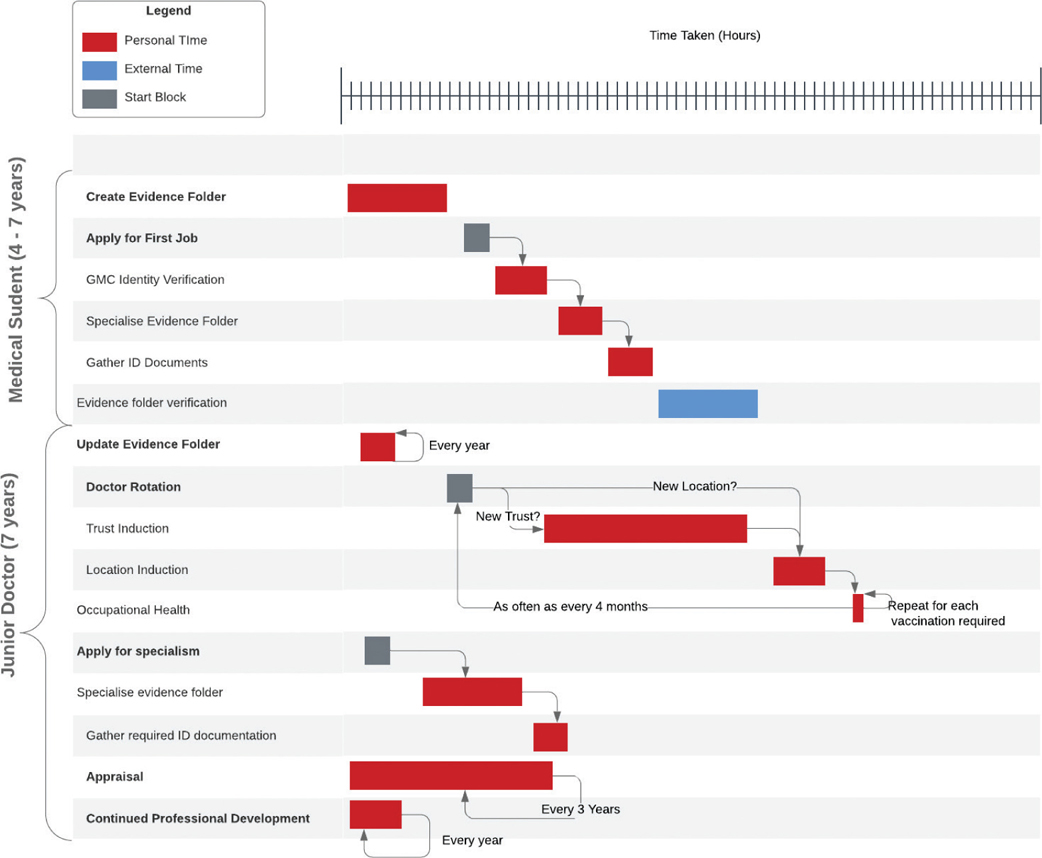
The workshop participants were split into groups, and each group focused on four of the identity moments. The results were then presented back to the group providing a detailed overview of each of the stages in a doctor’s career, including recurring and trusted ecosystem entities such as the GMC (General Medical Council). These maps were combined and synthesized into a Gantt chart, showing the time burden and repetition associated with healthcare professionals as they progress through their career, see Figure 2. This was developed through follow-up communication with a final year trainee at the RCPE who attended the workshop.
Figure 2—Healthcare professional’s identity moments.
The next stage of the workshop involved an interactive session on self-sovereign identity and the capabilities it could provide healthcare professionals when applied to the key identity moments that participants previously mapped out. The goal was to give attendees a high level understanding of how this technology works and where it might fit into existing processes within healthcare.
Physical props were used to represent different aspects of the SSI system, and a number of workshop attendees were asked to play roles within the healthcare ecosystem. Specifically, six participants acted as the key entities and trust providers identified in the process mapping stages:
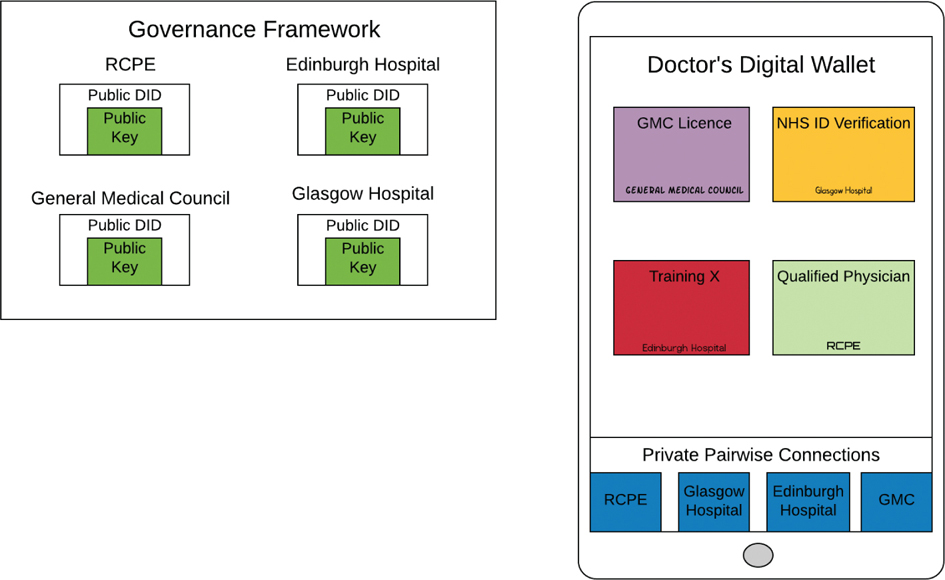
The initial setup of the SSI healthcare ecosystem was represented by asking each actor in the scenario to generate a public/private key pair. A red (private) and green (public) card was used to show the two halves of a public/private key pair. Actors then attached their public key to a white card, which was used to represent a decentralized identifier (DID). All actors were asked to place their DID onto the wall, representing the act of registering a public DID on a distributed ledger such that the public keys for these trusted entities could be resolved by anyone.
After the initial setup, a member of the research team played the role of doctor and walked through each of the identity moments discussed and mapped in the process mapping session. This interactive approach was used for a couple of purposes:
Throughout this interactive session, a flipchart was used to represent the doctors’ digital wallet. The wallet gradually collected verifiable credentials represented as large post-it notes and digital relationships, formed through peer DID connections, were represented as small blue post-it’s within the wallet (see Figure 3).
Figure 3—A illustration of the workshop’s physical representation of an SSI ecosystem.
Within an SSI system, there are generally four core interactions:
Each of these interactions was represented in this scenario as follows:
1. Establishing a peer DID connection: For this interaction, the action used was simply a handshake between the doctor and the party the doctor wished to connect with. For example, during the doctor qualifies from medical school process mapping, the doctor had to establish a connection with the GMC. While the handshake took place, participants were explained that this represented forming a private peer-to-peer communication channel across which message integrity and authenticated origin can be verified. It was illustrated that the connection was stored and managed by the digital wallet using a small blue post-it note.
The fact that these connections could be formed either face to face, or through a website, was additionally discussed. Explaining that you probably have more trust in a connection formed face to face and that trust can be built across these connections by sharing verifiable information.
This relationship once formed can last indefinitely, until one individual or the other decides to break it off. This means that the GMC or any entity could form more personal relationships with the doctors they license, enabling them to push them relevant communication across their secure communication channel.
2. Credential issuance: Credential issuance was a recurring SSI interaction that was represented in the scenario. The medical school issued the doctor their medical degree, the GMC issued their license, and the RCPE issued the doctors a qualified physician credential. All these credentials exist in the current system. They are attestations about the attributes and qualifications of a doctor, made by entities with the authority to make such claims. Before any credential issuance interaction, a secure connection must have been formed as discussed above this was highlighted through a handshake action.
Then workshop participants acting as the different trusted entities within the scenario were asked to write the name of the credential (a large post-it) and sign the credential using their private key—the red card they received as part of the setup. In reality, they used a wet signature to represent this. This helped convey the concept that once a credential has been signed it is impossible to change the contents of that credential without invalidating the signature—providing integrity to the credential.
For simplicity, the scenario did not represent individual attributes that credentials contained—for example, a GMC credential might contain the doctors’ name and their GMC license number. This was conveyed verbally instead.
During the session, the signature type—CL signatures, and the way that they work in the context of verifiable credentials was briefly touched upon, due to the importance to understand why a doctor couldn’t easily share a credential. Specifically, the doctor contributes some secret information in a blind manner into the signing protocol as one of the credential attributes. Such that when the credential is signed and given to the doctor, only they can prove they know the secret value that was signed by the issuer. Even the issuer does not know this.
The wall of trusted DIDs and their corresponding public keys was used to discuss how the doctors, or rather their wallets, could verify the signatures on any credentials they were issued to ensure they were valid. The doctor is also capable of refusing a credential or suggesting changes before accepting—for example, if the issuer had spelt his/her name wrongly.
3. Proof Request: A proof request is an SSI interaction whereby an entity, generally referred to as a verifier, requests proof of certain identity information from a holder—in this scenario the doctor. The verifier is able to additionally specify the credential schema that the identity information should come from and the credential issuer if they wish.
For example, in the ecosystem modeled there were only two hospitals—let’s call them Glasgow Hospital and Edinburgh hospital for simplicity, Edinburgh may request proof of a doctor’s name and DoB contained within an identity verification credential and only accept this proof if it was issued by Glasgow Hospital (represented by its DID).
This was a complex interaction that was challenging to represent within the scenario, so verbal communication was used to outline the majority of it. The actor representing the entity asking for a proof from the doctor wrote this request on a piece of card which was then passed to the doctor. It was made clear that this communication went across an already established DID connection and that proof requests could include a subset of attributes from across multiple credentials.
4. Credential presentation: A credential presentation was the final SSI interaction used repeatedly throughout the scenario. This is the process by which a doctor, through the use of their digital wallet, responds to a proof request by creating a cryptographic presentation from one of more verifiable credentials within their wallet.
Within the scenario, this was illustrated by filling out a card and creating a wet signature on this card. The card was then passed to the entity/actor who requested the proof request. Again, a lot of the complexity was conveyed verbally. It was explained that a credential presentation is not the same as giving the credential within a digital wallet to the entity requesting it. A presentation is a new and distinct cryptographic object that is created from one or more credentials and can contain any number of attributes from these credentials. This has both privacy and security benefits.
Going back to the hospital example, Edinburgh may request a doctor to prove his/her name, date of birth, and GMC license number when initially employing a new doctor. This proof request can be responded to in a single credential presentation that combines the attributes from two separate credentials originally issued by different entities into a new object that is still cryptographically verifiable using the public keys of the issuers, the keys that are publicly available and were stuck on the wall during the initial setup.
The last session of the workshop involved presenting SSI in the context of traditional identity management systems such as federated and user-centric identity management systems.
Then asking for positive and negative aspects of the SSI system presented to them, challenges to its implementation were also collected through this process.
After this, eight design principles and their definitions selected from the literature were presented to the group. Mentimeter, a tool for audience engagement, was used to gauge how the participants valued these design principles. A couple of additional questions were also asked.
Before we introduced the design principles from the literature to our audience, we asked them what they thought was the most important feature of future technology that would help them trust it. The list included the following:
Comparing this list with the list of design principles that we distilled from the literature demonstrates that our audience adds two specific principles to the generic list. The first is that they find it important to know that all entities will be involved in the SSI ecosystem, including the government and the NHS. The success of the system depends on buy-in of all of the involved entities and that is something that should be developed from the start. Second is the attention for usability and convenience. User engagement is important from the start and throughout the development process.
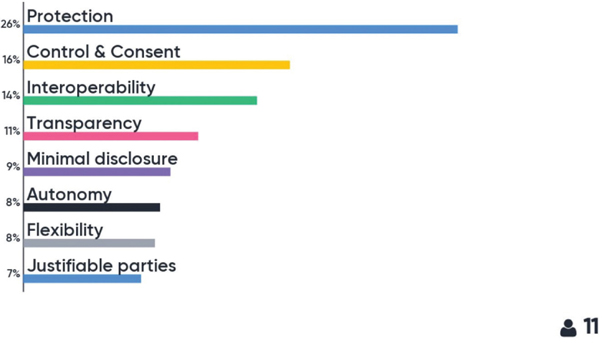
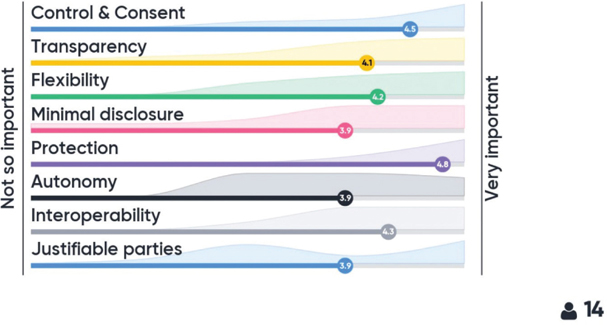
We selected eight principles from the literature and explained the definitions to the participants. Then, we asked them to rank the principles in order of importance. The majority selected protection as the most important, followed by control and consent and interoperability. Then, we asked to rank importance for each individual principle. Again, the highest scores were for protection, control and consent, and interoperability. Figures 4 and 5 show the results of the Mentimeter polls. This was used to get a sense of the room and the figures should be interpreted with that in mind.
Figure 4—Principles ranked by importance.
Figure 5—Principles individually rated.
The workshop led to a number of key learning elements about identity management for healthcare professionals. This can be generally summarized as being complex, fragmented, and time-consuming in its current form. The process mapping session led to an increased understanding of the identity landscape within healthcare. We began the session with eight identity moments that we framed as being chronological; the idea behind this was to provide a rough skeleton for participants to expand on in their process maps. It came to light that we missed a key identity moment within a doctor’s career, namely appraisal and re-validation. A process whereby healthcare professionals must prove to relevant authorities that they have gone through the relevant training to keep their skills up to date such that they can still practice. This is a repetitive process that occurs every 3 years. It was interesting to find out that even the top level professionals in attendance typically spent a couple of days every 3 years getting their documents in order for this procedure.
Another point of clarification was that while we positioned the eight identity moments as chronological, a lot of them happen in parallel. For example, a medical student typically gets identity checked by the GMC prior to graduating, and they also spend their final year applying for jobs so that on graduation they are ready to begin their career immediately. It was pointed out that there is no strict temporal relationship between the eight stages initially identified and a large part of the frustrations come from the fact that the majority of these stages are repeated over the course of a doctor’s career, each time requiring the same time-consuming procedure.
A good example of this comes from what we broadly termed doctor rotation, something commonly experienced within the healthcare system, especially for young doctors who can rotate to a new location and role as often as every 4 months. While this reduces significantly as doctors progress in their career, it is still a common occurrence. Every time a doctor moves to a new hospital, there are a number of tasks that the doctor needs to complete in order to on-board into the institution:
Another big bugbear of the group, particularly from attendees still going through training, was keeping track of all the training events they had attended, including the need to enter this information into multiple distinct silos. This was further exacerbated by frustrating user experiences, different document format requirements, and even reviewers specifically asking for physical copies due to the added burden that reviewing digitally uploaded documents entailed, a clear example of how digital tools have failed healthcare professionals by increasing rather than reducing the burden placed on them to manage their professional careers.
To summarize, the process mapping and ensuing discussions highlighted numerous frustrations experienced by healthcare professionals just to meet the requirements for managing their career. A phrase that came up was the need to professionalize the digital experience throughout a doctor’s career.
The method for conveying the capabilities of SSI and how these might change the identity moments a doctor experiences throughout their career was a success. The majority of participants were engaged and achieved a good level of understanding as shown through the questions that this generated. Many of the participants indicated that they would be receptive to these changes being implemented, in particular a trainee at the RCPE was very supportive.
The workshops additionally surfaced a number of challenges that attendees thought would need to overcome in order to roll this out within a healthcare system. Many participants were senior professionals within healthcare, so had experiences of other attempts to digitize aspects of healthcare. The three core challenges identified were:
To conclude, participants were largely in favor of the technology described in the workshop, at least from the viewpoint of its worth exploring further. A number of them were keen to be involved in further iterations, offering support finding additional doctors and medical students to further explore the requirements of any technical solution from their perspective. This research has further reinforced the importance of developing user-driven systems, ensuring that any solution that does get rolled out is meeting the actual needs of those it is designed for. The research identified overlooked design principles and also showed that the design principles commonly referred to within the academic literature, when explained, were also considered important by the system users within a healthcare context.
Next steps include developing a proof of concept which can then be validated with real users; this will include validating it against the properties deemed important by participants: Usability and security. Additionally, a medical student’s identity interactions in themselves seem complex, and it would be valuable to run another workshop specifically focusing on this area. This should provide a different perspective from that gained throughout this workshop.
The professionalization of the digital experience within a doctor’s career is long overdue. Furthermore, the COVID-19 crisis has highlighted just how important these solutions can be for the NHS and its individual trusts. Staffing needs fluctuate widely across the country, as different regions and hospitals hit their peaks of this crisis at different times. The ability to redeploy doctors to highly stressed areas within the NHin minutes rather than in days could greatly improve a health services ability to cope—see trust induction Figure 2. While a portion of these induction processes can perhaps be ignored, trusts still have to meet strict legal requirements around identity verification2—this all takes time which could be spent saving lives.
This seems to be the opportune moment to develop and deploy an SSI solution. However, it is imperative that any solution that is developed, especially if rushed through during a crisis, is clear about what it wants to achieve and for whom. Furthermore, these solutions should identify a process by which to validate how well they are meeting the predefined aims and requirements of those who are actually going to be using it—healthcare professionals.
The authors would like to extend their thanks to Dr Manreet Nijjar, an infectious disease consultant and co-founder of truu.id, a company working to realize much of what is discussed throughout this article. His attendance at the workshop was invaluable. Also thanks to Professor Derek Bell and Pernille Marqvardsen without whom this workshop would not have been possible.
There are no conflicts of interest.
There are no related funded projects.
| 1. | Regulatory overload. Tech. Rep. 10. American Hospital Association; 2017 [Internet] [cited 2020 May 01]. Available from: https://www.aha.org/system/files/2018-02/regulatory-overload-report.pdf |
| 2. | Ruscoe M. Identity verification and authentication standard for digital health and care services. Health and Social Care Information Centre; 2018, p. 19. |
| 3. | Holmes C. Distributed ledger technologies for public good: leadership, collaboration and innovation. House of Lords; 2018. |
| 4. | Keswani RN, Taft TH, Coté GA, Keefer L. . . Increased levels of stress and burnout are related to decreased physician experience and to interventional gastroenterology career choice: findings from a US survey of endoscopists. Am J Gastroenterol. 2011;106(10):1734. |
| 5. | Heponiemi T, Hyppo¨nen H, Vehko T, et al. Finnish physicians’ stress related to information systems keeps increasing: a longitudinal three-wave survey study. BMC Med Inform Decis Mak. 2017;17(1):147. [Internet] [cited 2020 May 01]. Available from: http://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-017-0545-y |
| 6. | Ferguson N, Laydon D, Nedjati Gilani G, et al. Report 9: impact of non-pharmaceutical interventions (NPIs) to reduce covid19 mortality and healthcare demand. Ageing and Mental Health; 2020. |
| 7. | Mettler M. Blockchain technology in healthcare: the revolution starts here.” 2016 IEEE 18th international conference on e-health networking, applications and services (Healthcom). IEEE, 2016; pp. 1–3. |
| 8. | Thouin MF, Hoffman JJ, Ford EW. The effect of information technology investment on firm-level performance in the health care industry. Health Care Manage Rev. 2008;33(1):60–8. |
| 9. | Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Affairs. 2008;27(3): 759–769. |
| 10. | Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573–576. |
| 11. | F. of State Medical Boards. Healthcare and digital credentials: technical, legal and regulatory considerations. Federation of State Medical Boards, Tech. Rep., 6. 2019. |
| 12. | Identity checks. Tech. Rep., 4. NHS Employers; 2019 [Internet] [cited 2020 May 01]. Available: https://www.nhsemployers.org/-/media/Employers/Publications/employment-check-standards/Identity-checks.pdf |
| 13. | Dyer C. Gmc checks 3000 doctors’ credentials after fraudulent psychiatrist practised for 23 years. NHS Employers; 2018. |
| 14. | Gallant J. The laws of identity. 2019 [Internet] [cited 2020 May 01]. Available from: https://www.thestar.com/news/gta/2019/07/31/expert-who-gave-more-than-100-assessments-in-ontario-child-protection-cases-lied-about-credentials-for-years-judge-finds.html |
| 15. | Goodman M. Dr death. 2016 [Internet] [cited 2020 May 01]. Available from: https://www.dmagazine.com/publications/d-magazine/2016/november/christopher-duntsch-dr-death/ |
| 16. | Federation credentials verification service. [Internet] [cited 2020 May 01]. Available from: https://www.fsmb.org/fcvs/ |
| 17. | Read TE. Clinical skills passport: a method to increase participation in clinical skills by medical students during a surgery clerkship. J Surg Educ. 2017;74(6):975–9. |
| 18. | Cser A. Forrester’s risk-driven identity and access management process framework. 2017. |
| 19. | Reed D, Sporny M, Sabadello M. Decentralized identifiers (DIDs) v1.0. Tech. Rep., 2019 [Internet] [cited 2020 May 01]. Available from: https://w3c.github.io/did-core/ |
| 20. | Connor-Green DS. Blockchain in healthcare data. Intell. Prop. & Tech. LJ. 2016;21:93. |
| 21. | Liang X, Shetty S, Zhao J, Bowden D, Li D, Liu J. Towards de-centralized accountability and self-sovereignty in healthcare systems. International Conference on Information and Communications Security. Springer, 2017; pp. 387–398. |
| 22. | Liang X, Zhao J, Shetty S, Liu J, Li D. Integrating blockchain for data sharing and collaboration in mobile healthcare applications. 2017 IEEE 28th Annual International Symposium on Personal, Indoor, and Mobile Radio Communications (PIMRC). IEEE, 2017; pp. 1–5. |
| 23. | Seppa¨nen R, Blomqvist K, Sundqvist S. Measuring inter-organizational trust—a critical review of the empirical research in 1990– 2003. Ind Market Manag. 2007;36(2):249–265. |
| 24. | van den Berg B, Keymolen E. Regulating security on the internet: control versus trust. Int Rev Law Comput Tech. 2017;31(2):188–205. |
| 25. | Smolenski N. The evolution of trust in a digital economy. 2018 [Internet] [cited 2020 May 01]. Available from: https://www.scientificamerican.com/article/the-evolution-of-trust-in-a-digital-economy/ |
| 26. | Cameron K. The laws of identity. 2005 [Internet] [cited 2020 May 01]. Available from: https://www.identityblog.com/stories/2005/05/13/TheLawsOfIdentity.pdf |
| 27. | Cameron K. The laws of identity on the blockchain. 2018 [Internet] [cited 2020 May 01]. Available from: https://www.youtube.com/watch?v=FvOQjTO6HI |
| 28. | Allen C. The path to self-sovereign identity. 2016 [Internet] [cited 2020 May 01]. Available from: http://www.lifewithalacrity.com/2016/04/the-path-to-self-soverereign-identity.html |
| 29. | Tobin A, Reed D. The inevitable rise of self-sovereign identity. The Sovrin Foundation. 2016;29(2016). |
| 30. | Dunphy, P, Petitcolas FA. A first look at identity management schemes on the blockchain. IEEE Security & Privacy 16(4):20–29, 2018. |
| 31. | Ferdous MS, Chowdhury F, Alassafi MO. In search of self-sovereign identity leveraging blockchain technology. IEEE Access. 2019;7:103 059–103 079. |
| 32. | van Bokkem D, Hageman R, Koning G, Nguyen L, Zarin N. Self-sovereign identity solutions: the necessity of blockchain technology. arXiv preprint arXiv. 2019;1904:12816. |
| 33. | Stokkink Q, Pouwelse J. Deployment of a blockchain-based self- sovereign identity. 2018 IEEE International Conference on Internet of Things (iThings) and IEEE Green Computing and Communications (GreenCom) and IEEE Cyber, Physical and Social Computing (CP- SCom) and IEEE Smart Data (SmartData). IEEE, 2018; pp. 1336–42. |
| 34. | Toth KC, Anderson-Priddy A. Self-sovereign digital identity: a paradigm shift for identity. IEEE Security & Privacy. 2019;17(3):17–27. |
| 35. | Spierings J, Demeyer T. Digitale Identiteit: een nieuwe balans? Amsterdam: De Waag Technology & Society, Tech. Rep., 2019 [Internet] [cited 2020 May 01]. Available from: https://digitaleidentiteit.waag.org/wp-content/uploads/sites/6/Wegingskader-digitale-identiteit.pdf |
| 36. | Schraffenberger H. IRMA made easy. 2020 [Internet] [cited 2020 May 01]. Available from: https://irma.cs.ru.nl/ |
| 37. | “Outdated” it leaves NHS staff with 15 different computer logins. 2020 [Internet] [cited 2020 May 01]. Available from: https://www.bbc.co.uk/news/health-50972123 |
Copyright Ownership: This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.